
Front-line erlotinib in unselected patients with advanced NSCLC and poor performance status - the TOPICAL study
Lung cancer has long been recognized as an extremely heterogeneous disease since its development, in terms of clinical characterizations, prognosis, response and tolerance to treatment, is unique in every patient. Eastern Cooperative Oncology Group performance status (ECOG PS) is the most important predictor of outcome in advanced non-small-cell lung cancer (NSCLC). Patients with PS ≥2 tend to tolerate treatment poorly and have significantly inferior survival compared with patients with PS 0 to 1 (1). As a result, patients with poor PS have historically been excluded from clinical trials, and scant evidence-based information is available to guide clinical practice. Studies evaluating the safety and efficacy of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors, such as erlotinib and gefitinib, have given rise to a remarkable degree of optimism based on prolonged remissions and improvements in quality of life in small numbers of patients whose condition no longer responded to standard chemotherapy (2,3).
The Lancet Oncology has featured this month the results of the TOPICAL trial, a double-blind, placebo-controlled phase III trial which investigated the use of erlotinib in NSCLC patients with poor PS and several co-morbidities (4). Seventy eight centers in the UK participated, and a total of 670 chemotherapy naïve patients with newly diagnosed, pathologically confirmed stage IIIB or IV NSCLC were involved (4). Patients were randomized to receive either erlotinib, 150 mg per day, or placebo until disease progression or unacceptable toxicity (4). The primary endpoint was overall survival. The trial began enrolling patients in 2005 and, as a result, EGFR mutation status was not used as an enrolment criterion (4). Patients were required to have been deemed unsuitable for chemotherapy because of poor PS (≥2), or the presence of several co-morbidities, or both, and have estimated life expectancy of at least 8 weeks (4).
Median overall survival did not improve with the use of erlotinib compared to placebo [erlotinib, 3.7 months, 95% CI, 3.2-4.2, vs. placebo, 3.6 months, 95% CI, 3.2-3.9; unadjusted hazard ratio (HR) 0.94, 95% CI, 0.81-1.10, P=0.46] (4). Adverse events reported showed that grade 3 or 4 diarrhea was more common with erlotinib than placebo [8% (28 of 334) vs. 1% (4 of 313), P=0.0001], as was high-grade rash [23% (79 of 334) vs. 2% (5 of 313), P<0.0001]; other adverse events were the same between the two groups (4). Among patients who received erlotinib, a subset analysis showed that development of rash during the first 28 days of treatment (first-cycle rash) was the only significant independent factor associated with improved overall survival (HR 0.76, 95% CI, 0.63-0.92, P=0.0058) and progression free survival (PFS) (HR 0.66, 95% CI, 0.54-0.80, P<0.0001) in a multivariate analysis (4). Compared with placebo, overall survival seemed to be worse in the group that did not develop first-cycle rash (HR 1.30, 95% CI, 1.05-1.61, P=0.017) (4). Lee and colleagues conclude that erlotinib prolongs overall survival in patients with NSCLC deemed unsuitable for chemotherapy, but only in those who develop first-cycle rash, whereas those who do not have a rash after 28 days should discontinue erlotinib, due to the possibility of decreased survival (4).
In the accompanying study of potential biomarkers of sensitivity to erlotinib, DNA was available from 390 of the 398 patients who provided material (58% of total study population) (4). Seven percent (27/390) of patients had an activating EGFR mutation, a low mutation rate which can be attributed to the fact that almost 40% of the randomized patients had squamous NSCLC and only 5.5% of them did not have a history of smoking (4). The benefits of erlotinib were observed regardless of EGFR status. KRAS mutations (19%, 73/390) were neither prognostic nor predictive of erlotinib benefit (4).
TOPICAL is an interesting study looking at erlotinib for the treatment of patients with newly diagnosed advanced NSCLC who are not sufficiently fit to undergo treatment with chemotherapy. However it raises intriguing questions about the treatment of patients with PS 2 and the mechanism underlying a selective benefit for patients who develop first-cycle rash.
A limitation of this study, which the investigators acknowledge, is the inclusion of patients with ECOG PS 2. For such patients, results of a previous study showed better PFS with chemotherapy compared to erlotinib (HR 1.45, 95% CI, 0.98-2.15, P=0.063) (5). Fifty-six percent (372 of 670) of the TOPICAL study population had PS 2 and many oncologists would recommend conventional chemotherapy to these patients.
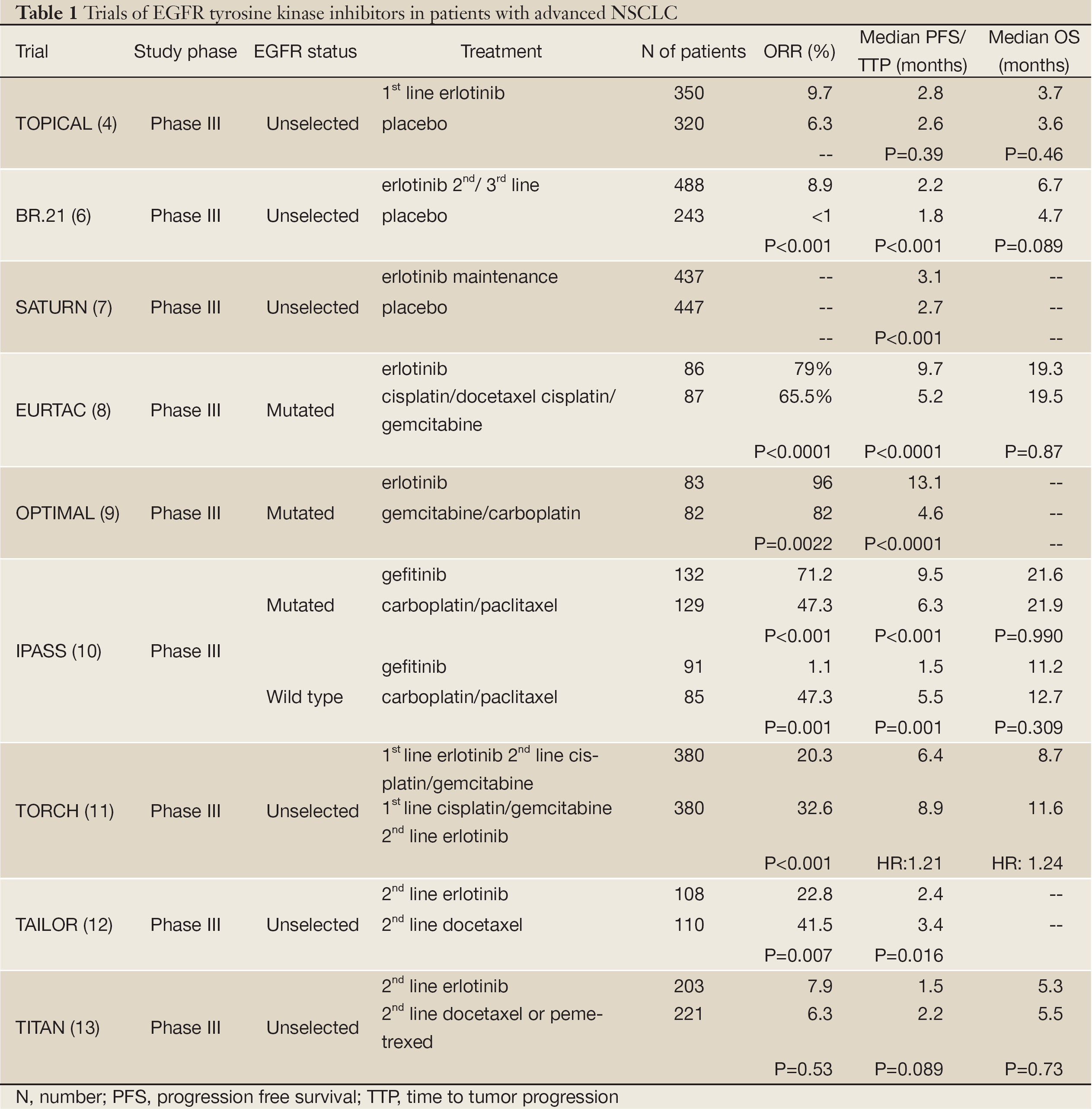
In practice, oncologists do sometimes consider erlotinib for patients who are not candidates for chemotherapy, or who refuse this treatment. When erlotinib was compared to placebo, in unselected patients with advanced NSCLC pretreated with standard first-line or second-line chemotherapy, such as the BR.21 or SATURN study, a survival advantage was clearly shown (Table 1) (6,7). However, EGFR tyrosine-kinase inhibitors are best used in patients with EGFR mutant tumors for whom the strongest evidence of benefit exists (8,9). The Tarceva or Chemotherapy study (TORCH) compared first line erlotinib followed by second-line chemotherapy with initial chemotherapy followed by erlotinib, irrespective of EGFR genotype (11). The study was stopped early because of inferiority of first-line erlotinib in unselected patients, providing convincing evidence that those patients are harmed by foregoing first line chemotherapy, even if it is planned for them to receive the same treatment opportunities in due course (11). These findings reinforce the results seen in the IRESSA Pan-Asia Study (IPASS), where patients with clinical characteristics suggestive of response but without an EGFR mutation had longer PFS with carboplatin and paclitaxel than with an EGFR tyrosine-kinase inhibitor (10). Finally, second line docetaxel was found to be superior to erlotinib in an EGFR wild-type population with a PFS HR of 0.70 (95% CI, 0.53-0.94, P=0.016), as presented in the Tarceva Italian Lung Optimization tRial (TAILOR) (12). The Tarceva In Treatment of Advanced NSCLC study (TITAN) was the first trial to show that erlotinib has comparable efficacy to chemotherapy (docetaxel or pemetrexed) and is better tolerated in hard-to-treat unselected NSCLC cases, where cancer has progressed on or immediately after treatment with first-line therapy (Table 1). Although Tudor Ciuleanu and colleagues concluded that outcomes for patients treated with erlotinib or chemotherapy did not differ, there have been several criticisms of this trial and its conclusions (13).

Full table
Patients treated with EGFR inhibitors frequently develop rash characterized by inflammatory papules and pustules on the scalp, face, neck, and upper torso. The incidence of rash ranges from 50% to 100%, depending on the agent and cancer type, and median onset is typically within 1 to 2 weeks of starting therapy (14). An overview of all phase II erlotinib studies by Perez-Soler et al., showed a correlation between rash severity and response and survival, while Wacker et al., after analyzing data from two large phase III studies (NCIC CTG Study BR.21 and NCIC CTG Study PA.3), suggested that rash from erlotinib is associated with improved outcomes (15,16). However, rash cannot be predicted before treatment initiation, limiting its usefulness as a predictive marker. In the TOPICAL study, erlotinib improved overall survival in patients who developed first-cycle rash (HR 0.76, 95% CI, 0.63-0.92, P=0.0058). The relationship between rash, erlotinib dose and response has not been fully elucidated. Molecular analysis of skin and tumor tissue samples collected before and after therapy as part of an ongoing ECOG phase II study of single-agent erlotinib in patients with NSCLC will hopefully provide answers to some of these questions. One possible explanation is that, although skin rash may require effective target inhibition, it occurs primarily as a result of the patient’s ability to mount an immune-mediated inflammatory response. Thus, rash may be a surrogate of immunocompetence rather than receptor inhibition and would be difficult to incorporate into routine practice as a predictive marker. Erlotinib-induced rash is not present before treatment, and after initiation of treatment other markers, such as radiographic response and clinical benefit, are more likely to accurately predict outcomes.
The TOPICAL study has failed to demonstrate an overall survival benefit of erlotinib in an unselected group of patients with advanced NSCLC who are too frail to cope with chemotherapy. The most common adverse event with the EGFR tyrosine kinase inhibitor was rash, which was found to be a surrogate for predicting response and possibly survival. However, prospective investigation is needed to elucidate the correlation between outcomes with erlotinib and rash and, for now, rash should not be used as a marker for erlotinib response in clinical practice, since insufficient data exist. Moreover, EGFR wild-type patients with adequate PS, including ECOG PS 2, seem to have better outcome when treated with cytotoxic chemotherapy. Further studies are needed to augment the benefit of erlotinib in EGFR wild-type patients when the option of traditional chemotherapy is exhausted. Until we have a biological explanation for tyrosine kinase inhibitor activity in EGFR wild-type patients, restricting use of erlotinib to those most likely to respond - i.e., patients carrying specific molecular or clinical characteristics - is advisable. When the TOPICAL study was designed, EGFR mutation status was not used as an enrolment criterion. However, since then we have moved forward to the era where most NSCLCs are defined as EGFR-positive or EGFR-negative and the era of a single treatment for all is now in the past.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- Lilenbaum RC. Treatment of advanced non-small-cell lung cancer in special populations. Oncology (Williston Park) 2004;18:1321-5; discussion 1326, 1329-33.
- Kris MG, Natale RB, Herbst RS, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer: a randomized trial. JAMA 2003;290:2149-58.
- Pérez-Soler R, Chachoua A, Hammond LA, et al. Determinants of tumor response and survival with erlotinib in patients with non--small-cell lung cancer. J Clin Oncol 2004;22:3238-47.
- Lee SM, Khan I, Upadhyay S, et al. First-line erlotinib in patients with advanced non-small-cell lung cancer unsuitable for chemotherapy (TOPICAL): a doubleblind, placebo-controlled, phase 3 trial. Lancet Oncol 2012;13:1161-70.
- Lilenbaum R, Axelrod R, Thomas S, et al. Randomized phase II trial of erlotinib or standard chemotherapy in patients with advanced non-small-cell lung cancer and a performance status of 2. J Clin Oncol 2008;26:863-9.
- Shepherd FA, Rodrigues Pereira J, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med 2005;353:123-32.
- Cappuzzo F, Ciuleanu T, Stelmakh L, et al. Erlotinib as maintenance treatment in advanced non-small-cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncol 2010;11:521-9.
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol 2012;13:239-46.
- Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol 2011;12:735-42.
- Fukuoka M, Wu YL, Thongprasert S, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol 2011;29:2866-74.
- Gridelli C, Ciardiello F, Gallo C, et al. First-line erlotinib followed by second-line cisplatin-gemcitabine chemotherapy in advanced non-small-cell lung cancer: the TORCH randomized trial. J Clin Oncol 2012;30:3002-11.
- Garassino MC, Martelli O, Bettini A, et al. TAILOR: a phase III trial comparing erlotinib with docetaxel as the second-line treatment of NSCLC patients with wildtype (wt) EGFR. Proc Am Soc Clin Oncol 2012;30:abstr LBA7501.
- Ciuleanu T, Stelmakh L, Cicenas S, et al. Efficacy and safety of erlotinib versus chemotherapy in second-line treatment of patients with advanced, non-small-cell lung cancer with poor prognosis (TITAN): a randomised multicentre, open-label, phase 3 study. Lancet Oncol 2012;13:300-8.
- Segaert S, Van Cutsem E. Clinical signs, pathophysiology and management of skin toxicity during therapy with epidermal growth factor receptor inhibitors. Ann Oncol 2005;16:1425-33.
- Pérez-Soler R, Chachoua A, Hammond LA, et al. Determinants of tumor response and survival with erlotinib in patients with non--small-cell lung cancer. J Clin Oncol 2004;22:3238-47.
- Wacker B, Nagrani T, Weinberg J, et al. Correlation between development of rash and efficacy in patients treated with the epidermal growth factor receptor tyrosine kinase inhibitor erlotinib in two large phase III studies. Clin Cancer Res 2007;13:3913-21.


{kind=link}